



Gender Dysphoria and Darwinism
Gender Dysphoria and Darwinism
by Dr Jerry Bergman
The belief that some people are born in bodies of the wrong sex was challenged by a recent scientific study claiming this condition amounted to what the researchers termed “rapid onset gender dysphoria.” Dysphoria means “a state of dissatisfaction, anxiety, restlessness, or fidgeting”—a disorder, in other words, implying an unnatural state, as opposed to euphoria, “a state of intense happiness and self-confidence.”
The finding would appear to agree with Genesis 1:27 and 2:24, quoted by Jesus, who said, “From the beginning of the creation, God ‘made them male and female. … For this reason a man shall . . . be joined to his wife, and the two shall become one flesh.”[2] In contrast to this view, many evolutionary theorists accept the idea of gender fluidity, namely the view “that gender is not fixed by biology, but shifts according to social, cultural, and individual preference.”[3]

In the image of God He made them; male and female He created them. Genesis 1:27 (Credit: AiG Creation Museum)
Based on passages similar to the scriptures quoted above, Judaism, Christianity, and Islam have always taught the concept of gender complementarity—the view that God designed men and women for different, but corresponding, social roles. Acceptance of Darwinism negates this constraint as shown by the fact that families who hold to Genesis usually don’t have to confront this issue, because they accept the view that God “made them male and female,” and look for other solutions for indications of gender dysphoria.[4]
Darwinist, by contrast, evaluate “human male and female behavior and that of animals, which like our own, have evolved over time.” From this, they rationalize gender diversity, concluding that evolution can explain gender fluidity as a particular social, genetic, or environmental consequence of natural or sexual selection.[5] Evolutionist Sally Hines supports the evolutionary view of gender fluidity in detail by analyzing human evolution, asserting that our evolutionary ancestors did not hold to the modern traditional binary male and female gender roles.[6]
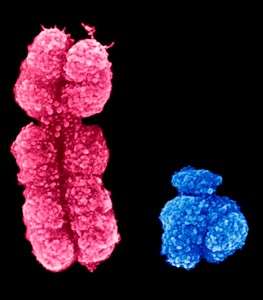
X and Y chromosomes differ dramatically in size, structure and content
The Genesis teaching is supported by observational evidence. Both biological and psychological evidence supports the gender-complementarity view of traditional male and female roles.[7] Males and females display biological differences from the zygote stage to birth and also after birth. Except for red blood cells, which are enucleated (lacking a nucleus), every healthy normal human body cell is either male (containing XY chromosomes) or female (XX chromosomes). Given the average human contains 50 trillion cells, depending on his or her weight, each person has over 100 trillion male and female X Y chromosomal differences. So-called gender reassignment cannot change these differences.
A Psychological Problem
Historically, the belief that some men were trapped in a female body and some women were trapped in a male body was seen as a psychological problem—not a biological one. It required psychotherapy or counseling, not surgery. Instead of agreeing with the male’s contention that he was a woman trapped in a male body, the historical approach was counseling – to deal with the dysphoria (mental dissatisfaction) based on a false, non-biological belief or feeling. A ‘transgender male’ feels she actually is a male, and desires body changes to match her self-perception, and vice versa. Before the current LGBT movement, counselors sought to alleviate the dysphoria by helping the person accept and enjoy (euphoria) their biological sex.
We’re not talking about biological matters, but rather feelings. The concern here is not a documented genetic problem, such as Pseudo-hermaphroditism, a general term I learned in medical school but which is no longer used. Genetic terms are now preferred because they describe the specific medical condition, such as 5-α-reductase deficiency and androgen insensitivity syndrome. Most cases of Pseudo-hermaphroditism are caused by one or more mutations.[8]
Social Science Research
Anthropological studies have consistently found that “in every sort of society, using every sort of approach—scientists are finding differences in the way men and women organize their verbal and visual-spatial abilities. The studies do not always agree with one other exactly,” allowing for some, but limited, cultural influence. [9] One of the most detailed studies of male and female differences titled The Great Divide compiled over 2,000 differences between males and females documented by scientists, sociologists, psychologists and government agencies. The differences included biological, psychological, sociological, economic, political and religious.[10]
The trendy new practice of “gender reassignment” is so new that very few studies on the problem have been completed. One of the most complete was done by Brown University Professor Lisa Littman, MD. Her peer-reviewed study was approved by a University ethics committee and published in a peer reviewed academic journal. She found that youth peer influence was an important factor leading some teens to believe that they are suffering from gender dysphoria, which in turn can lead them into life-changing cross-sex hormone treatments or even surgery, such as mastectomies, a response which many young people have come to regret.[11]
When a young girl comes to believe she is a male trapped in a female body, for example,
Many clinicians and therapists oblige—at least with hormones—and they persuade parents to go along by using frightening leverage: They warn the alternative could be suicide. Terrified parents often give in.”[12]
The fact is, suicide is a problem both many youth who are gender dysphoric (believe they are in the wrong body) as well as gender-transitioned persons face. The rate of suicide attempts among transgender people is very high, even after they “transition” into the opposite sex.
Littman received 256 responses to her request from parents about their teenage children who had no previous signs of gender dysphoria and who, out of the blue, declared they were suffering from gender dysphoria. More than 85 percent of the survey respondents said they support gay marriage, indicating the parents likely weren’t concerned about their child’s declaration of transgenderism for religious reasons. That the concern is not biological is supported by the fact that over 60 percent of the parents noted their “child had been diagnosed with a mental health disorder before claiming gender dysphoria, suggesting the teens needed help, but perhaps for other underlying problems.”[13]
Dangers of Gender Reassignment
The solutions for gender reassignment include hormone therapy, surgery, and counseling, but not necessarily in that order. Except anabolic steroid hormones, little is known in detail about long term use of high doses of powerful male and female hormones. After the transition, stopping the hormones results in a number of problems, such as the reappearance of many traits common to the birth sex. Thus, hormone therapy will likely be a life-long obligation. In the case of anabolic steroid treatment, the results have been tragic and likely the same is true of long-term androgen and estrogen hormone therapy. There are no long-term studies to prove this is necessary, safe, or prudent treatment—but there are many well documented hazards to using these same hormones when treating adults for medical conditions.
Once the teenage years begin, “affirmative care” involves giving young people cross-sex hormones regardless what the parents wish. Girls younger than 12 are prescribed testosterone for lifetime usage, while boys are given estrogen. These are serious hormonal treatments that impact brain development, cardiovascular health, and may increase the risk of cancer. Transgender declarations tend to occur in clusters by group suggestion, similar to how groups of teenage girls will suddenly develop eating disorders concurrently.
In the next segment, Dr Bergman will discuss additional research findings about gender, and describe how the media and progressives distort the science.
References
[1] Littman, Lisa. 2018. Parent reports of adolescents and young adults perceived to show signs of a rapid onset of gender dysphoria. PLOS One. August 16 pp. 1-44.
[2] Mark 10:6-8.
[3] Hines, Sally. 2018. Is Gender Fluid. London: Thanes & Hudson. p. 6.
[4] Interview with Professor M. Blank.
[5] Hines, 2018, pp. 23-26.
[6] Hines, 2018, pp. 28-30.
[7] Alumkal, A. W. 2017. Paranoid Science: The Christian Right’s War on Reality. New York: New York University Press. 107-108.
[8] McPhaul Michael J. and James E. Griffin 1999. Male Pseudo hermaphroditism Caused by Mutations of the Human Androgen Receptor. The Journal of Clinical Endocrinology & Metabolism, 84(10): 3435–3441. 1 October.
[9] Durden-Smith, Jo and Diane DeSimone.1983. Sex and the Brain. New York: Arbor House. p. 42.
[10] Weiss, Daniel Evan. 1991. The Great Divide. New York: Poseidon Press.
[11] Singal, Jesse. 2018. When Children Say They’re Trans. Hormones? Surgery? The choices are fraught—and there are no easy answers. The Atlantic. July-August.
[12] Dean, Jamie. Rapid-onset Gender Dysphoria: This year’s social Contagion infects teenagers and their Doctors. World Magazine.34(3):34-39.
 Dr. Jerry Bergman has taught biology, genetics, chemistry, biochemistry, anthropology, geology, and microbiology at several colleges and universities including for over 40 years at Bowling Green State University, Medical College of Ohio where he was a research associate in experimental pathology, and The University of Toledo. He is a graduate of the Medical College of Ohio, Wayne State University in Detroit, the University of Toledo, and Bowling Green State University. He has over 1,300 publications in 12 languages and 40 books and monographs. His books and textbooks that include chapters that he authored, are in over 1,500 college libraries in 27 countries. So far over 80,000 copies of the 40 books and monographs that he has authored or co-authored are in print. For more articles by Dr Bergman, see his Author Profile.
Dr. Jerry Bergman has taught biology, genetics, chemistry, biochemistry, anthropology, geology, and microbiology at several colleges and universities including for over 40 years at Bowling Green State University, Medical College of Ohio where he was a research associate in experimental pathology, and The University of Toledo. He is a graduate of the Medical College of Ohio, Wayne State University in Detroit, the University of Toledo, and Bowling Green State University. He has over 1,300 publications in 12 languages and 40 books and monographs. His books and textbooks that include chapters that he authored, are in over 1,500 college libraries in 27 countries. So far over 80,000 copies of the 40 books and monographs that he has authored or co-authored are in print. For more articles by Dr Bergman, see his Author Profile.