



Scientists Were Wrong About Tooth Cavities
Another Case of Scientists Being Proved Wrong:
Cavities are not caused by bad bacteria but by the loss
of a complex, well-designed bacterial ecosystem.
by Jerry Bergman, PhD
Once upon a time the claim that “science supports” something was all the evidence required to prove a point. As I wrote on December 23, 2021 about fluoridation of water, settled science has become ‘unsettled’ several times recently. As a result of these reversals—plus the coronavirus debacles of 2020 and 2021—many people’s confidence in “science” has now been severely shaken.[1] Claims of mainline science are being questioned in other areas as well. Here is another case involving teeth. In addition to the reversal in advice about water fluoridation, a traditional theory of the cause of tooth decay has come under scrutiny.
Poor Design? No
The idea human teeth are poorly designed is an oft-repeated evolutionary notion as the cause of cavities. In an example from 2018 posted at Today’s Dental, the network of Omaha Dentists asked, “Why do we have so many problems with our teeth?” They complained that our “choppers are… riddled with cavities” and added, with an evolutionary flair, “It hasn’t always been this way.” They claim that our teeth didn’t evolve for modern society. “Dental problems such as crowding and cavities are common in people today,” they wrote. “But other species tend not to have such afflictions, nor did our fossil forebears.” Problems with teeth are attributed to evolution, they continue:
In many ways, human teeth are a marvel.… enamel is the hardest substance in the human body. And yet, humans often struggle with teeth that are misaligned, overcrowded, misshapen, discolored, and prone to decay. Most of us have dealt with a need for some sort of dental work, whether it be braces, fillings, extractions, or just a general cleaning. Sometimes it’s like no matter how hard humans try to care for our oral health, our teeth just commonly have problems. But why? In this blog post we take a closer look at human teeth and how they have evolved…. Hence, part of the reason we experience oral health issues is due to evolution.[2]
 Answering the Evolutionary Angle
Answering the Evolutionary Angle
I will show that this evolutionary-based view is incorrect. In fact, the findings of properly completed research argue for quite the opposite conclusion.
I learned in medical school that Streptococcus mutans was adept at attaching itself to hard tooth surfaces. It thrived on dietary sugars, and churned out acid that carved holes into our tooth enamel, causing tooth decay. Furthermore, I was taught that bacteria thrived in the acidic milieu that Streptococcus mutans produced. We were also taught that oral biofilms always damaged dental health.
Based on this commonly-taught maxim, dentists good recommended the elimination of as many oral bacteria as possible – ideally all of the bacteria in the oral cavity – for good oral hygiene. I also taught these conclusions to my college students for years.
All of these ideas have now been proven to be wrong.
History of Bad Dental Experimentation
Some history of how these beliefs were arrived at will be helpful in understanding how science often really works, which is not how it should work. In short, the
bacterium Streptococcus mutans was first implicated in causing dental caries in 1924, when an English dentist named J. Kilian Clarke found this microorganism at the scene of a cavity and declared it the culprit. Because the bacterium was easy to culture and study outside the mouth, scientists in subsequent decades were able to gather more and more evidence to support the guilty verdict: S. mutans was adept at attaching itself to hard tooth surfaces; it loved dietary sugars; and it churned out acid — in fact, it thrived in the kind of acidic milieu that carved holes in tooth enamel. By 1960, many dentists considered S. mutans the cause of dental caries (tooth decay) and by the mid-1970s, scientists were developing a caries vaccine from whole bacterial cells.[3]
The fact that scientists were developing a vaccine to treat the problem of tooth decay indicates how confident they were in their theory about the cause of cavities. The history of the development of this theory reveals much about the tenuousness of their theory. No comparison between the wide variety of oral bacteria and their potential contribution of the tooth cavity problem was carried out. Most importantly, Koch’s postulate of disease causation was totally ignored. Koch’s postulate should have been followed to determine if a specific bacteria caused a specific disease. The method is as follows:
- The bacteria must be present in every case of the disease.
- The bacteria must be isolated from the host with the disease and grown in pure culture.
- The specific disease must be reproduced when a pure culture of the bacteria is inoculated into a healthy susceptible host.
- The bacteria must be recoverable from the experimentally infected host.[4]
In 1890, bacteriologist Robert Koch published his now celebrated criteria for judging if a given bacteria is the cause of a specific disease. His criteria brought much-needed scientific clarity to what was then a very confused field and what is today the standard for identification of causal agents.
The Vaccine Fails
It turned out the vaccine they were developing did not work: “Little did these researchers know that the vaccine was misdirected. It turned out that S. mutans was not acting alone to cause dental damage. It was receiving assistance from other microbial cells.”[5] The researchers decided to apply the scientific method to the problem, specifically Koch’s 1890 postulates. To do so they cultured bacteria taken from several sites in the mouth of patients and “studied the characteristics of specific bacteria, leading them to pin oral diseases on certain microbes.”
Fortunately, at this time new gene-sequencing techniques were available, along with innovative imaging tools, allowing careful research on the details of the oral cavity microbiome. The results drastically changed “long-held views about how microbes contribute to dental health.”[6] In short, they found, in contrast to “settled science,” that the
members of the microbial population remain constant, despite a regular influx of microbes that enter the mouth during eating, breathing or nail biting. Not all microbes survive in the oral environment, but the average person has around 250 species from a pool of around 700 documented oral residents. These species can evade the anti-microbial defenses of saliva.
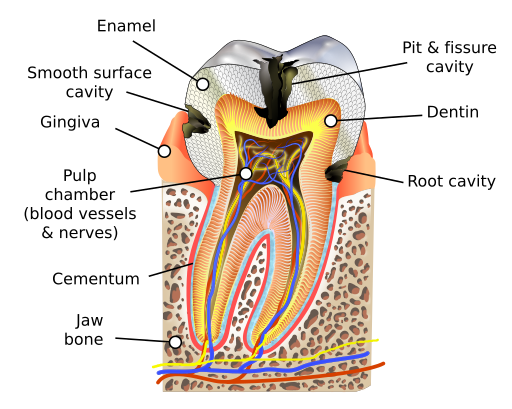
Cross section of a tooth showing decay in three places. From Wiki Commons.
A Revolutionary New View
One of the most important findings was that the old consensus about problematic species of bacteria invading the mouth, requiring mouthwash to kill as many bacteria as possible, was not only wrong, but the exact opposite was true. Specifically,
the oral microbiome is not a homogeneous collection of life forms, but rather an assortment of mini microbiomes [are located] at different sites in the mouth. The microbes seem to be specialists for the niche that they occupy, whether … saliva or dental plaque, or other areas of the oral cavity: tongue, cheek, palate, throat or tonsils. Different places in the mouth that are only millimeters apart from each other are inhabited by completely different microbial communities.[7]
A new picture has emerged. Each appropriate species of bacteria must travel to the proper niche, thrive there, and work together with other oral bacteria in the mouth as a team. Dental plaque is a biofilm composed of self-assembling microorganisms assembling into an arrangement resembling a hedgehog:
Filamentous bacteria had stacked on top of each other to build a main spiny structure, with other organisms nestled in between the spikes. This happened in a healthy mouth … the microbial species composition, as well as the biofilm’s physical structure, change in the transition from health to disease.[8]
Because the former scientific consensus is wrong, it has now been replaced by a very different one, as explained by University of Amsterdam oral microbial ecologist Egija Zaura, who related
that during her dental training in the early 1990s, she was taught that oral biofilms were always bad. Now that view has changed — it seems the effect depends on which microbes the biofilm contains. Zaura says that given the clear benefits of brushing on oral health, wiping out the biofilms through regular brushing (for people who consume lots of starches and sugars, at least) must have positive overall effects on the oral microbiome. [9]
The only way to explain this long-term stability of the microbe community is by a new theory: the health-promoting microbes present in the biofilm rapidly grow back after brushing to protect the teeth from their next acid bath. Uzel et al. showed that after a professional dental cleaning people with periodontitis gum disease grow a different biofilm with an higher number of certain microbial species.[10]
Specifically, supragingival plaque counts of Veillonella parvula, Fusobacterium nucleatum ss vincentii, and Neisseria mucosa increased between 2 to 7 days. These are only a few of the bacterial colonies that research indicates are part of the favorable protective bacterial biofilm. Now it is known that Streptococcus salivarius helps to control the oral inflammatory response.[11] Other bacteria convert urea to ammonia to balance the oral pH. Some bacteria even produce products to help control oral pathogens that cause cavities.
Thus, bacteria that have a role in causing cavities, are reduced by certain other bacteria. Specifically Streptococcus dentisani produces antimicrobial molecules that kill Streptococcus mutans.[12] Some oral microbes transform the nitrate produced from fruits and vegetables into nitrite, which is then converted into nitric oxide, a critical blood-pressure regulator that causes vasodilation.
Summary: A Healthy Ecosystem
This review only begins to cover the important roles of oral bacteria. Seeing the oral microbiomes as cooperating teams has revolutionized our understanding of oral health. For example, scientists now know that many over-the-counter antiseptic mouthwashes destroy beneficial microbes and interfere with the crucial roles they play in maintaining good dental health. Especially problematic are mouthwashes containing chlorhexidine that kill microbes. This revolution in oral health was described by one researcher as follows:
ten years ago the predominant thinking in dentistry was that people needed to keep the oral cavity ‘clean’ by getting rid of as many oral bacteria as possible. But this is now seen as folly — a 2020 study showed that healthy people who rinsed with chlorhexidine mouthwash experienced a major shift in their salivary microbiomes, leading to more acidity in the mouth and lower nitrite availability, with a trend toward higher blood pressure.[13]
Consequently, changes in the oral microbial community allows bacteria that are normally kept under control by other microbes as part of a healthy ecosystem to become virulent. The result is oral disease. This new knowledge is a drastic shift from the simple “‘bad bacteria’-secretes-acids-that-cause-cavities” belief that lasted for almost a century causing untold levels of harm.
Editor Comment: Cavities, gum disease and other dental problems are still realities that destroy teeth, which were created to last a lifetime. One should not think that consuming large amounts of sugar is now acceptable, or that brushing and flossing are no longer needed. The point Dr Bergman makes is that assumptions and experiments without appropriate rigor can lead to wrong ideas about causation. Moreover, simplistic theories can endure in a scientific consensus for a century or more! Dental hygienists need to move beyond the notion of “bad bacteria” and learn how the microbial ecosystems in the mouth contribute to health or disease. You might want to share Campbell’s article with your dentist.

Teeth are incredibly well designed and should last a lifetime. Graphic by David Coppedge.
References

How to lose respect for evolutionary scientists. Look what crazy ideas the scientific consensus promoted in the past!
[1] Bergman, Jerry. 2021. “Settled Science” Unsettled: The Case of Fluoridated Water. Another case of scientific consensus has been undermined. How many were put at risk by a false idea? https://crev.info/2021/12/settled-science-unsettled-the-case-of-fluoridated-water/, December 23.
[2] Today’s Dental. 2018. Why Do Humans Have Weak Teeth? https://omahadentists.net/blog/humans-weak-teeth/, November 30.
[3] Campbell, Kristina. 2021. Oral microbiome findings challenge dentistry dogma. Nature https://www.nature.com/articles/d41586-021-02920-w, October 27.
[4] Stöppler, Melissa Conrad. 2021. Medical definition of Koch’s postulates. MedicineNet https://www.medicinenet.com/kochs_postulates/definition.htm, last reviewed on March 29.
[5] Campbell, 2021.
[6] Campbell, 2021.
[7] Campbell, 2021.
[8] Campbell, 2021.
[9] Campbell, 2021.
[10] Uzel, Naciye G., et al. 2011. Microbial shifts during dental biofilm re-development in the absence of oral hygiene in periodontal health and disease. Journal of Clinical Periodontology 38(7):612–620.
[11] Kaci, G., et al. 2014. Anti-inflammatory properties of Streptococcus salivarius, a commensal bacterium of the oral cavity and digestive tract. Applied Environmental. Microbiology 80(3):928–934.
[12] Scannapieco, Frank A., et al. 2001. Oral bacteria and respiratory infection: Effects on respiratory pathogen adhesion and epithelial cell proinflammatory cytokine production. Annals of Periodontology 6(1):78-86, December; Scannapieco, Frank A., et al. 1999. Role of oral bacteria in respiratory infection. Journal of Periodontology 70(7):793-802, July.
[13] Campbell, 2021.
 Dr. Jerry Bergman has taught biology, genetics, chemistry, biochemistry, anthropology, geology, and microbiology for over 40 years at several colleges and universities including Bowling Green State University, Medical College of Ohio where he was a research associate in experimental pathology, and The University of Toledo. He is a graduate of the Medical College of Ohio, Wayne State University in Detroit, the University of Toledo, and Bowling Green State University. He has over 1,300 publications in 12 languages and 40 books and monographs. His books and textbooks that include chapters that he authored are in over 1,500 college libraries in 27 countries. So far over 80,000 copies of the 40 books and monographs that he has authored or co-authored are in print. For more articles by Dr Bergman, see his Author Profile.
Dr. Jerry Bergman has taught biology, genetics, chemistry, biochemistry, anthropology, geology, and microbiology for over 40 years at several colleges and universities including Bowling Green State University, Medical College of Ohio where he was a research associate in experimental pathology, and The University of Toledo. He is a graduate of the Medical College of Ohio, Wayne State University in Detroit, the University of Toledo, and Bowling Green State University. He has over 1,300 publications in 12 languages and 40 books and monographs. His books and textbooks that include chapters that he authored are in over 1,500 college libraries in 27 countries. So far over 80,000 copies of the 40 books and monographs that he has authored or co-authored are in print. For more articles by Dr Bergman, see his Author Profile.