



Autism, Acetaminophen, and Human Genetic Health
Critics may prefer silence until
proof arrives. But silence is also a
policy choice—with consequences
by Ron Fritz, PhD
Introduction: Why This Debate Exploded
There has been growing debate in recent years about the safety of taking painkillers during pregnancy—especially acetaminophen (Tylenol)—and whether its use may be linked to autism in children. That debate reached a boiling point on September 22, 2025, when President Trump and Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. held a White House press conference announcing a new federal effort to “understand the causes of autism.”
During the press conference, autism was described as an “epidemic,” with officials stating that rates have surged nearly 400% since 2000 and now affect roughly 1 in 31 American children. They also suggested that acetaminophen may bear “substantial blame” for rising autism rates. As a result, the FDA announced changes to acetaminophen labeling and guidance to physicians, urging caution in its use during pregnancy unless medically necessary.
The reaction was immediate and fierce. Here are a few of the headlines that appeared within hours:
- “Scientific evidence is lacking to support the US government’s decisions to caution against using a common painkiller in pregnancy …” — New Scientist, Grace Wade, Sept 23, 2025
- “‘Highly concerning’: Major medical groups react to Trump’s claim that Tylenol is linked to autism” — ABC News, Sept 22, 2025
- “Trump links autism to Tylenol and vaccines, claims not backed by science” — Reuters, Sept 22, 2025
- “‘Sick to My Stomach’: Trump distorts facts on autism, Tylenol, and vaccines, scientists say” — KFF Health News, Sept 2025
The message from much of the press was clear: the administration had gone too far, too fast, and without solid evidence.
So, what’s really going on here? Why is this so controversial? And where does the truth actually lie? Let’s take it step by step.
Has Autism Really Reached “Epidemic” Levels?
According to the CDC, whose surveillance system is recognized worldwide as the most comprehensive for tracking autism in the United States, prevalence has risen from about 1 in 150 children in 2000 to 1 in 31 children by 2022. This corresponds to an average increase of roughly 6–8% per year1.
Other parts of the world show similar trends, though generally not as steep:
- Europe: ~3–5% per year2
- Asia: ~2–6% per year3
- Australia: ~4–7% per year4
So yes—autism rates have risen dramatically across the globe.
But here’s a key caveat: this does not automatically mean there is a true biological explosion of autism. Over the same period:
- Diagnostic criteria have broadened
- Screening has improved
- Awareness has increased
- Record-keeping has gotten better
All of these can inflate reported rates without any change in underlying biology. In plain terms: prevalence is up, but we don’t know how much of that increase reflects new biological cases.
A Double Standard About “Certainty”
This uncertainty cuts both ways. In her New Scientist article criticizing the administration, Grace Wade writes confidently:
“There is no crisis – rates of autism began to increase rapidly in the 1980s as diagnostic criteria for the condition expanded.”
But that statement is also not proven. Diagnostic changes explain some of the increase, but no one can currently say—with scientific certainty—that they explain all of it. Claiming “there is no crisis” requires the same level of certainty that critics accuse the administration of lacking.
In other words, certainty is being selectively applied. Calling autism an “epidemic” may be premature. But declaring that there is no biological increase at all is equally unsupported.
Does Uncertainty Mean We Shouldn’t Investigate Causes?
Even if we don’t know how much autism is truly increasing biologically, that doesn’t mean we shouldn’t try to understand its causes. Autism exists. It affects millions of families. Understanding what contributes to it—genetically, environmentally, or medically—is worthwhile regardless of whether prevalence is rising 2%, 5%, or not at all.
Using dramatic language at a White House press conference may have guaranteed attention—and scrutiny—but the core mission itself is hard to oppose.
What About Acetaminophen and Autism?
This is where things get more heated. The administration suggested that acetaminophen may contribute to autism risk when used during pregnancy. Critics immediately responded that such claims were “not backed by science.”
But the reality is more nuanced. Grace Wade herself acknowledges in her article that the literature is mixed:
“A recent analysis of 46 studies found 27 of them identified a significant association between using paracetamol (acetaminophen) in pregnancy and children having a higher risk of neurodevelopmental conditions such as autism.”
That’s not a fringe finding—but it’s also not definitive proof. Some studies show an association; others do not. How can both be true?
Why These Studies Conflict
All studies examining acetaminophen use during pregnancy are observational. That means researchers observe what people do; they do not assign treatments. Observational studies cannot prove causation because of confounding factors:
- Pregnant women take acetaminophen for fever, infection, pain, inflammation, stress, or autoimmune conditions
- Many of those same factors may independently affect fetal brain development
You can’t ethically run a study where pregnant women are randomly assigned to take a drug suspected of causing harm. Yet many critics, including Grace Wade, apparently demand proof of causality before any recommendations are made—something that, in this case, is impossible to achieve. Observational evidence is still valuable; it just needs to be interpreted carefully, with an understanding of its limitations.
So, What Should Public Health Officials Do?
This is the real policy dilemma.
One option is to wait for absolute proof of causality—but in this case, that proof may never come. The other option is to apply a precautionary principle: if a widely used medication might increase risk—and alternatives or limits exist—warn people while acknowledging uncertainty. HHS chose the second path.
The FDA explicitly stated that:
- Evidence is conflicting
- Causality is unproven
- Untreated fever also carries risks
- Acetaminophen should be used only when needed, at the lowest effective dose
This is not a ban. It is not a declaration of certainty. It is a warning under uncertainty. Critics may prefer silence until proof arrives. But silence is also a policy choice—with consequences.
Autism and Broader Genetic Health Trends
Autism is not alone. Many genetically influenced conditions and diseases appear to be rising at rates that go beyond what improved detection alone can explain. Estimates of biologically plausible increases include:
- Rheumatoid arthritis in adults 20–54: nearly doubling over the last 35 years (~0.62% per year)5
- Inflammatory bowel disease: 0.20–0.38% per year6
- Multiple sclerosis: 0.22% per year7
- Type 1 diabetes in young adults: 1.76–1.86% per year7
- Several early-onset cancers:
- Colorectal cancer in young adults: 2.0–2.9% per year8
- Liver cancer in young adults: 0.5–2.4% per year8
- Endometrial (uterine) cancer: 2.45–3.53% per year8
- Breast cancer: 0.29–0.78% per year8
- Leukemia: 0.94–2.44% per year8
- Melanoma (‘trunk’): women 3.5–4.4%, men 5.2–5.9% per year9
These figures suggest that for many conditions, true biological incidence is rising, not just reported diagnoses. Autism, while receiving the most attention, fits into a broader pattern of rising genetically influenced conditions—hinting at long-term changes in population health and genetic risk.
Are We Seeing Declining Genetic Health?
Evidence strongly suggests that our overall genetic fitness is declining. In other words, the accumulation of mutations over generations appears to be catching up with us, contributing to the rising prevalence of genetically influenced conditions and diseases we observe today.
Alexey Kondrashov, one of the world’s leading authorities on human genetics, famously writes:
“We should all be dead already!”
This statement underscores how sensitive humans are to mutation accumulation—particularly if we assume Homo Sapiens have existed for roughly 300,000 years. Peer-reviewed estimates suggest that genetic fitness declines by 1–2% per generation10, with more recent analyses placing it as high as 3–5% per generation11. Over hundreds of thousands of years, these rates would make long-term survival virtually impossible.
However, applying the same rates to genetically “perfect” humans, created 6,000 years ago, fits remarkably well with observed trends today (see plot below). It appears that the accumulation of mutations may be coming to a head, helping explain the rising prevalence of autism, autoimmune conditions, and other genetically influenced diseases we observe.
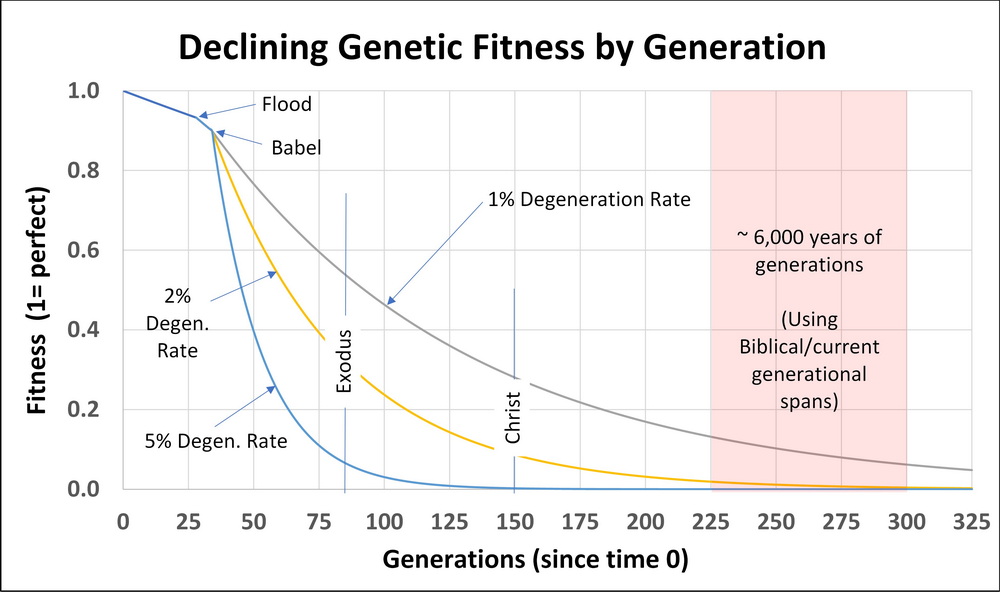
Time embellished version of Figure 4 from Genetic Entropy by Dr John Sanford (see ref 12).
Final Thoughts
Autism deserves serious attention. Prenatal acetaminophen exposure may be one of many contributing risk factors—but causality remains unproven. Because perfect certainty may never be attainable, HHS has chosen caution over inaction, recommending prudent use of acetaminophen during pregnancy. The truth about autism and acetaminophen sits in an uncomfortable middle ground: the evidence is suggestive, incomplete, yet still important to consider.
It’s fair to acknowledge that some of the administration’s language may have overstated confidence. But dismissing the issue entirely—or insisting on impossible standards of proof—is equally misguided and unhelpful.
Lastly, these debates highlight a broader context: our human condition. Rising rates of genetically influenced diseases—including autism—point to longer-term trends in our genetic health and remind us of our time and place in history and what lies ahead.
References
- S. Centers for Disease Control and Prevention. Data and statistics on autism spectrum disorder (ASD). CDC Autism and Developmental Disabilities Monitoring (ADDM) Network, 2025.
- Elsabbagh M, Divan G, et al. The global prevalence of autism spectrum disorder: a comprehensive systematic review and meta-analysis. Italian Journal of Pediatrics. 2022; 82(1): 1–17.
- Sun X, Allison C, et al. Prevalence of autism spectrum disorder in Asia: A systematic review and meta-analysis. Psychiatry Research. 2020;284:112679.
- Elsabbagh M, Divan G, et al. The global prevalence of autism spectrum disorder: a comprehensive systematic review and meta-analysis. Italian Journal of Pediatrics. 2022; 82(1): 1–17.
- Zhang, Z., Gao, X., Liu, S. et al.Global, regional, and national epidemiology of rheumatoid arthritis among people aged 20–54 years from 1990 to 2021. Sci Rep 15, 10736 (2025). https://doi.org/10.1038/s41598-025-92150-1
- Li, C. J., et al. (2024). Global burden of inflammatory bowel disease, 1990–2021: Evidence from the Global Burden of Disease Study 2021.
- Gong, B., Yang, W., Xing, Y. et al.Global, regional, and national burden of type 1 diabetes in adolescents and young adults. Pediatr Res 97, 568–576 (2025). https://doi.org/10.1038/s41390-024-03107-5
- Kehm RD, Yang W, Tehranifar P, Terry MB. 40 Years of Change in Age- and Stage-Specific Cancer Incidence Rates in US Women and Men. JNCI Cancer Spectr. 2019 Jun 10;3(3):pkz038. doi: 10.1093/jncics/pkz038. PMID: 31414075; PMCID: PMC6686848.
- Changing epidemiology and age-specific incidence of cutaneous malignant melanoma in Lithuania: an analysis of national cancer registration data by gender and anatomical site, 1991–2015.
- Crow, J. F. (1997). The high spontaneous mutation rate: Is it a health risk? Proceedings of the National Academy of Sciences of the United States of America, 94(16), 8380–8386. https://doi.org/10.1073/pnas.94.16.8380
- Lynch, M. (2010). Rate, molecular spectrum, and consequences of human mutation. Proceedings of the National Academy of Sciences of the United States of America, 107(3), 961–968. https://doi.org/10.1073/pnas.0912629107
- Sanford, J. C. (2014). Genetic entropy. FMS Publications. ISBN: 978‑0981631608

Ronald D. Fritz, PhD, is a retired research statistician whose career spanned 27 years. Before entering the field of statistics, he worked as an engineer and engineering manager in the defense industry. He earned his doctorate in Industrial Engineering, with a minor in Mathematical Statistics, from Clemson University, where he was honored as a Dean’s Scholar.
Dr. Fritz served as a consulting statistician across a broad range of industries, culminating in a 12-year role as a global statistical resource at PepsiCo. During his time at PepsiCo, he led significant research on gluten contamination in oats and its relationship to celiac disease, publishing several articles on the subject.
In retirement, Dr. Fritz developed a deep interest in creation science, sparked by a visit to the Creation Museum in Petersburg, Kentucky. As he delved into the topic, he shared his findings with his pastor, which led to an invitation to speak at their church. This initial presentation opened the door to further speaking engagements at churches throughout the region.
Dr. Fritz has been married for 35 years to his wife, Mitzie. They live in the mountain community of Bee Log, North Carolina, within sight of the church where they were married and now worship. In his free time, Dr. Fritz tends a small chestnut orchard on their property, working to revive what was once a cherished local delicacy. The couple has two adult children.
Comments
This discusses exactly what Dr. Sanford did in his 2006 book Genetic Entropy.
✅